Allen’s Tale
Allen’s Tale


My wife and I were out shopping when we came across a designer kitchen showroom. We were not in the market for a new kitchen but it is always nice to dream so we went in.
It was an Aladdin’s cave of state of the art kitchen technology and innovation. A gentleman came over and asked if he could assist us. We said we were only looking and dreaming, which he was fine with but went on to show us more. He was the owner and passionate about kitchens. He led us to his office and proceeded to show us a selection of virtual kitchens on his pc and explained how he could create a virtual design for us. At this point he asked me what I did for a living and I told him I was a dental technician. He instantly forgot about kitchens and started to explain how his teeth were the bane of his life. He was in constant pain, could not eat or speak properly and then he uttered the words “I would give anything to sort out my teeth”.
I could see as we talked that he had a remaining lower right canine and upper left canine, both of which were over erupted and mobile (Fig 1a). He also had a set of poor fitting unaesthetic dentures (Fig 1b). I felt sure I could help him and told him so. His response was that if I could sort out his teeth he would build us the kitchen of our dreams in gratitude
Initial Treatment
I referred him to one of my clients and so our tale begins. After an initial examination it was agreed that the two remaining teeth needed to be extracted.. It was decided in the first instance to fabricate a set of F/F immediate dentures, extract the remaining two teeth in order to provide a more aesthetic, better fitting, functional dentition.
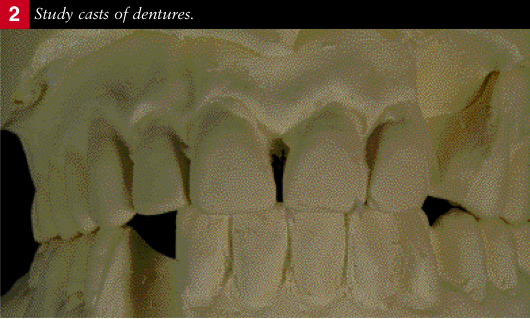
Impressions were taken without the dentures from which study casts were fabricated and mounted on a semi adjustable articulator using his existing dentures as a jaw registration. Shade and tooth mould were also selected. Impressions were taken of the existing dentures as a guide (Fig 2)
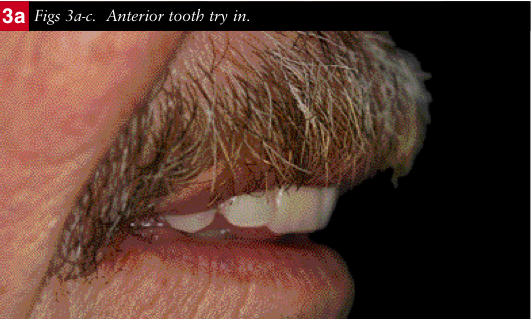
The anterior teeth were set up for a try in. Adjustments to the position of the teeth were carried out intraorally around the remaining canines. The mid line, smile line, incisal plane and lip support were all checked (Figs 3a-c). Once we were happy with the aesthetics the canines were removed from the casts, the rest of the teeth set up and immediate F/F dentures fabricated.
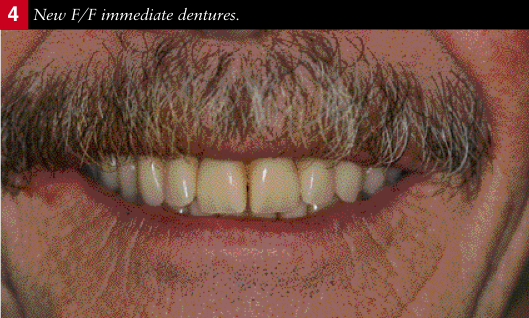
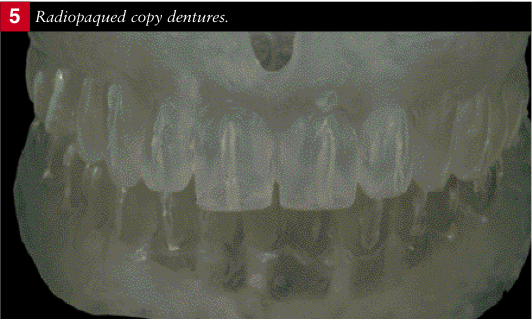
The remaining teeth were extracted and the dentures fitted (Fig 4). Whilst the tissues were healing and Allen was getting used to the dentures clear radiopaqued copy dentures were made (Fig 5). At the next visit the radiopaque dentures were used in conjunction with a CT scan to assess the relationship of the residual bone to the established tooth position on the dentures.
Sufficient residual bone in the mandible ensured that enough implants could be placed for fixed bridgework. Unfortunately there was insufficient bone in the maxilla and without the willingness to have sinus grafts it was decided to restore with a milled bar and integral attachments on four implants in combination with a removable prosthesis.


Implant Placement
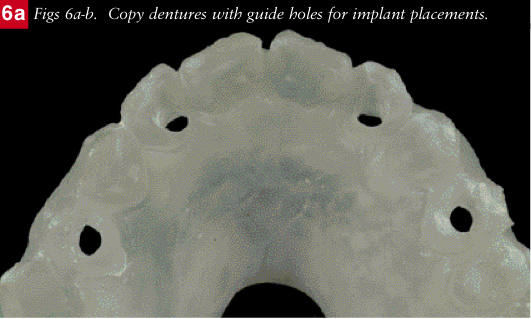
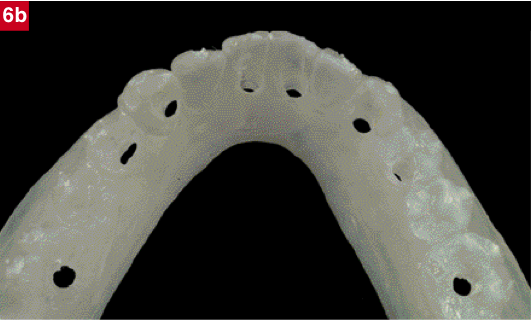
Using the information from the CT scans, holes were drilled into the clear copy dentures in what were considered to be the best positions for fixture placement and these were subsequently used as implant placement guides (Figs6a-b).
Eight implants were placed in the mandible and four in the maxilla. The dentures were selectively relieved to accommodate the healing caps on the fixtures. The dentures then continued to be worn throughout the healing and integration period.
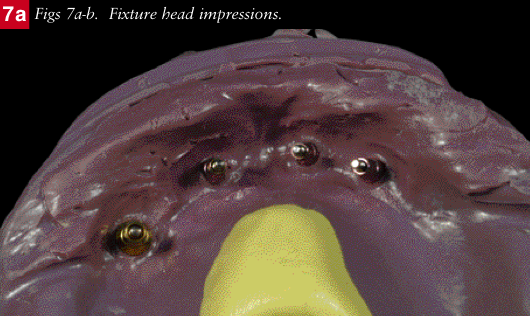
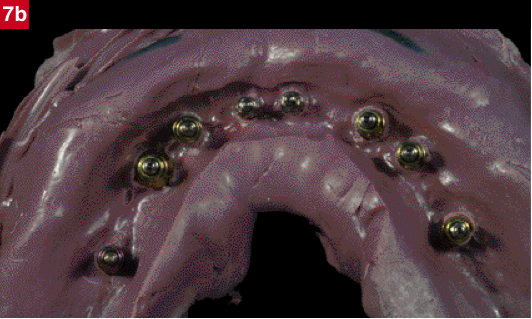
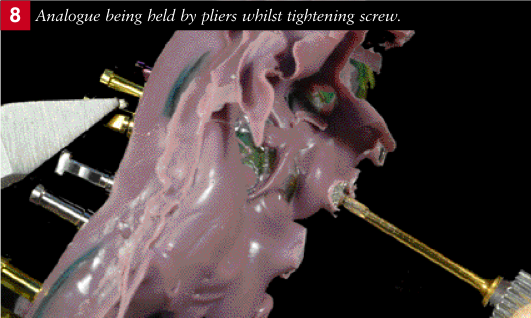
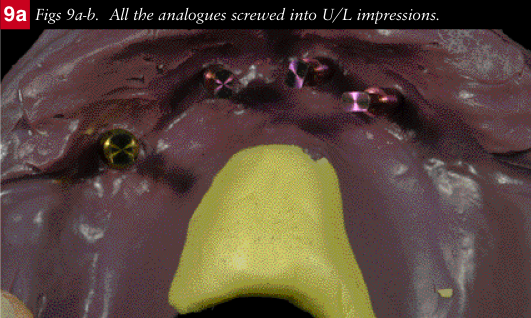
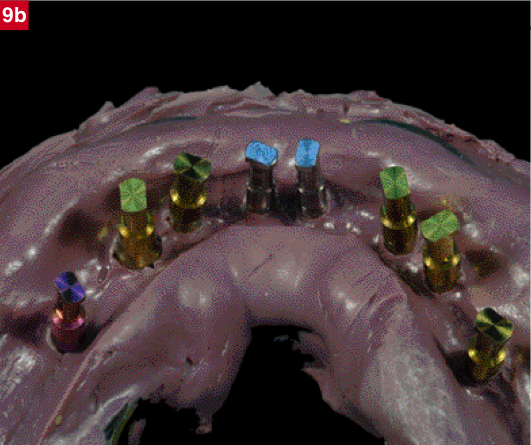
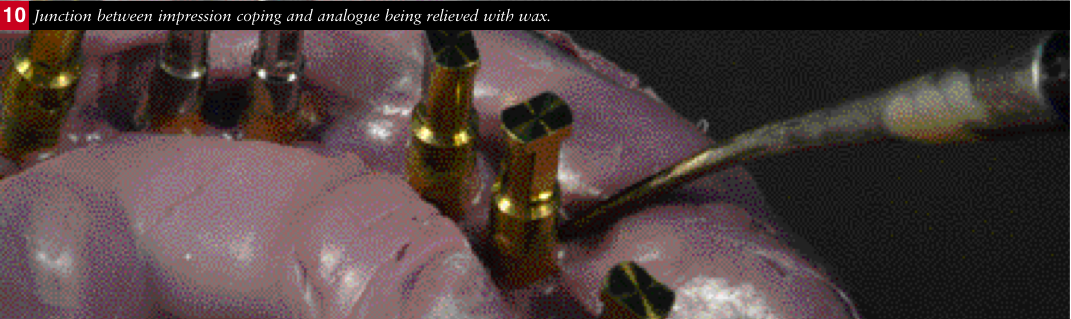
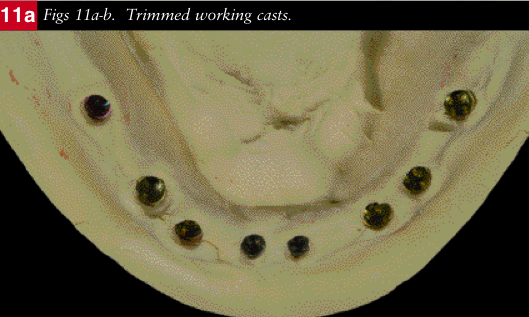
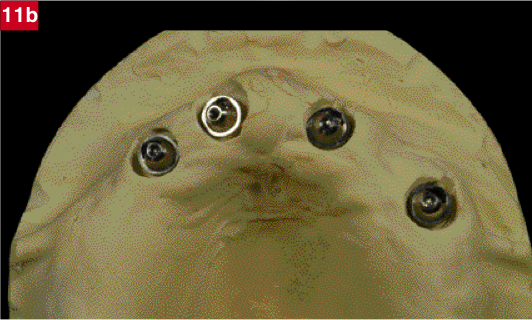
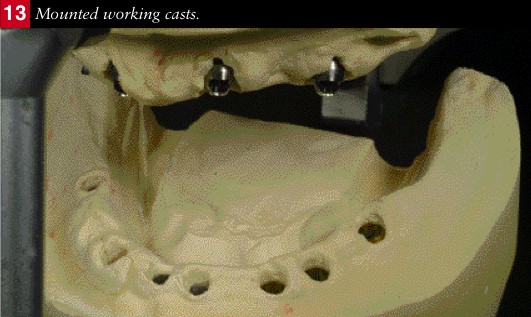
After six months the implants were uncovered and pick up impressions were taken (Figs 7a-b). Analogues of the fixtures were screwed onto the impression copings. Pliers were used to hold the analogues in order to prevent movement of the impression coping within the impression whilst tightening the screws (Fig 8). Once all the analogues had been secured (Figs 9a-b), a wax spacer was applied around the junctions of the impression copings and the analogues (Fig 10) to ensure subsequent ease of removal of the impression from the cast and good access to the heads of the analogues once the cast had been poured. Once the fixture head working casts had been fabricated (Figs 11a-b), the copy dentures were used as a jaw registration (Fig12) in order to mount the casts on a semi adjustable articulator (Denar Mk II) (Fig 13).

Definitive restorations
Indices were made from the dentures to establish the tooth position on the casts.
Upper Arch
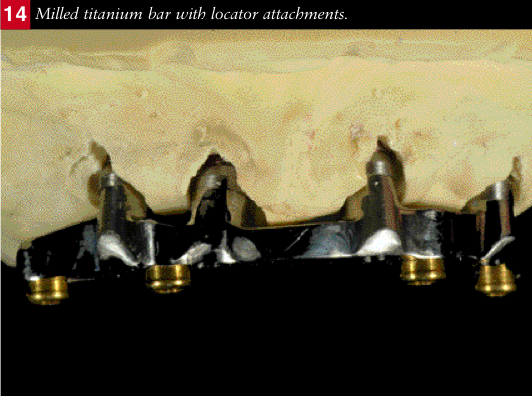
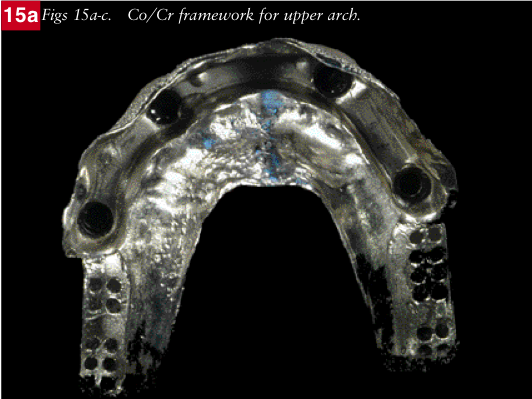
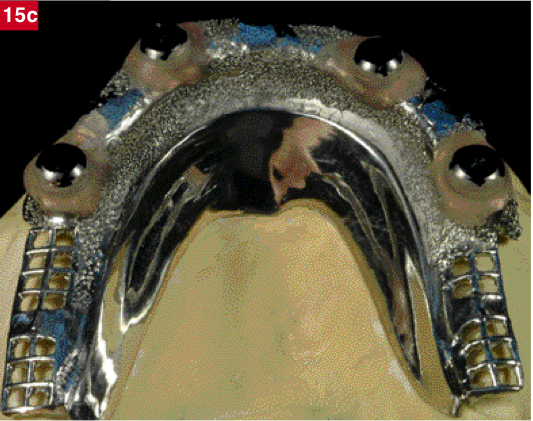
The upper working cast and index were sent to NobelBiocare who manufactured a titanium beam with integral locator attachments (Fig14). A Cr/Co denture framework was then constructed over the beam with housings for the locator attachments (Figs15a-c).
Lower Arch
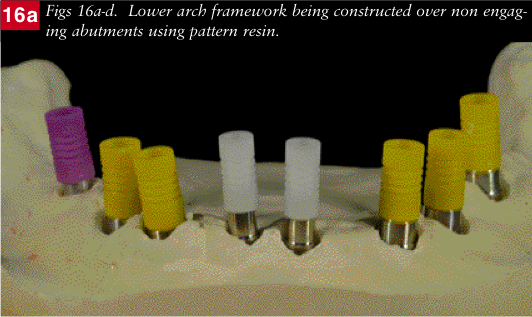
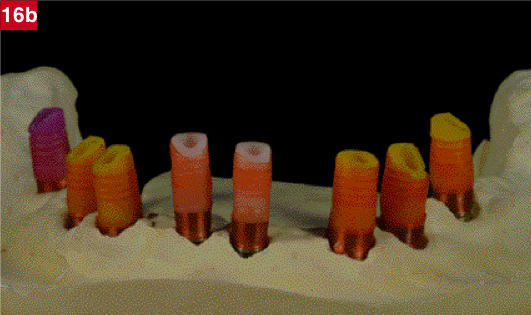
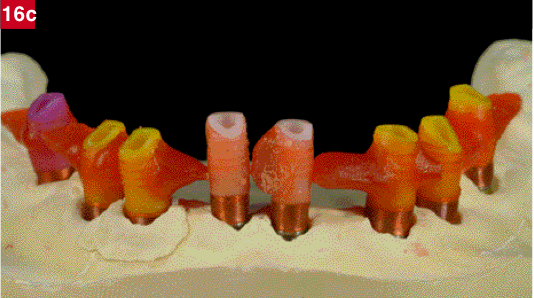
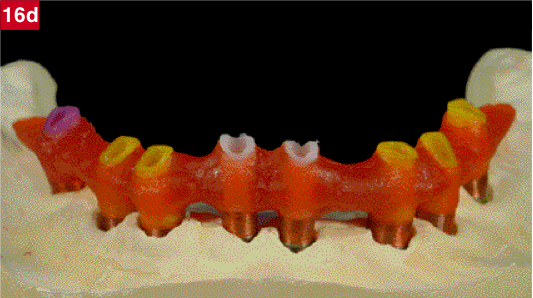
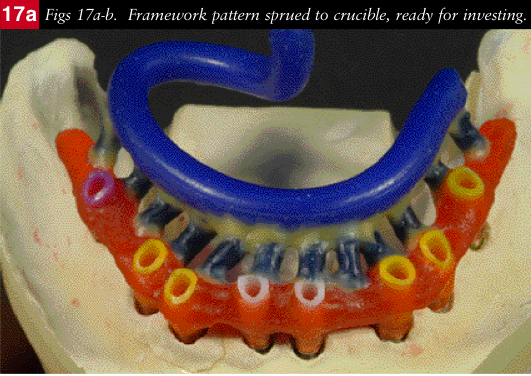
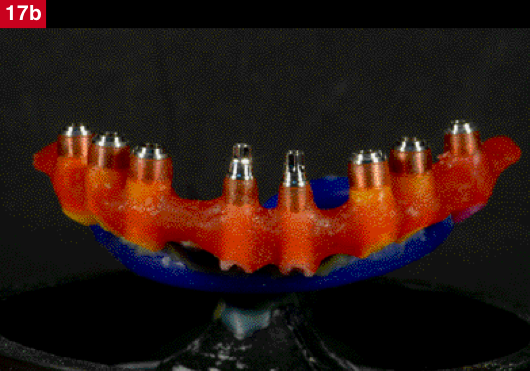
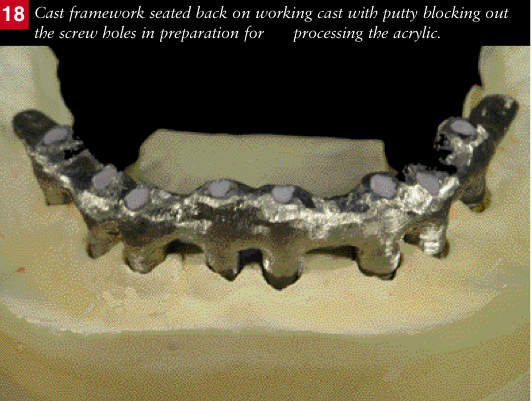
Non- engaging abutments (NobelBiocare-Conical Connect) were screwed to the lower working cast. A framework was fabricated around them with a pattern resin (GC) using the index of the tooth position as a guide (Figs 16a-d). The pattern was sprued and fixed to a crucible former for investing (Figs 17a-b). The framework was cast in a silver palladium alloy (Palliag M-Degudent). It was devested, trimmed and screwed to the working cast. The screw holes were then sealed with silicone putty to prevent resin locking in the screws when processing (Fig18).
A new set of denture teeth (Premium-Heraeus Kulzer) were then set up to the Co/Cr framework on the upper and the metal framework on the lower using the index as a guide.
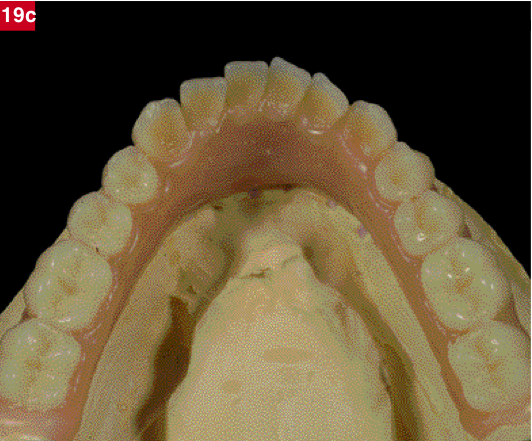
The tooth set up between the upper and lower arches were then adjusted and refined on the articulator and finally the soft tissues were waxed up to completion (Figs 19a-c).



Processing
The upper denture was removed from the model, invested and processed using the flask and packing technique.
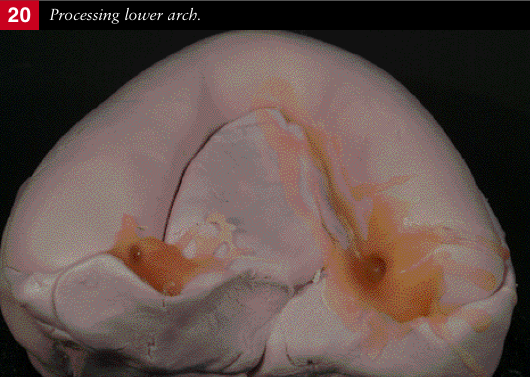
A silicone putty mould was made over the lower set up and used to process the arch. The putty mould was removed and access and exit holes made at each end for pouring the acrylic resin. The teeth were removed and all residual wax cleaned off with boiling water. The teeth areas to be set in the acrylic were then sandblasted with 90 micron aluminium oxide to ensure a good bond. The teeth were then seated back in the mould and where necessary, if the teeth were loose they were secured with a tiny drop of Cyanoacrylate. The mould was painted with a separator (Unifol) and the metal framework was treated with a bonding agent (Metafast). The mould was then seated back on the working cast and sealed around its periphery with further putty. Autopolymerising acrylic resin (Palapress-Heraeus Kulzer) was poured into the mould and cured in a pressure pot of water at 55 degree centigrade at 2 bar pressure for 10 minutes (Fig 20). On removal from the pressure pot the mould was cooled down under cold running water. The excess acrylic was removed with a tungsten carbide burr and the putty seal and mould carefully peeled off.
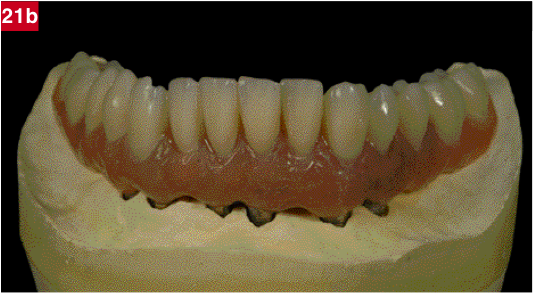
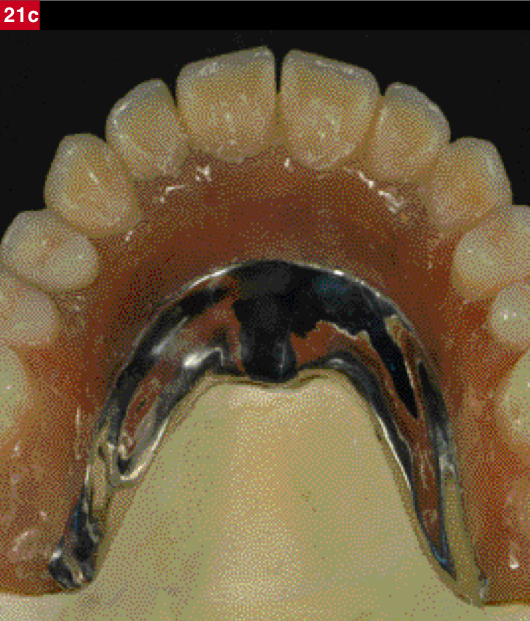
The processed upper denture and lower bridge in situ on their respective working casts were placed back on the articulator and the bite adjusted using red marking tape (12 micron) (Figs 21a-d).

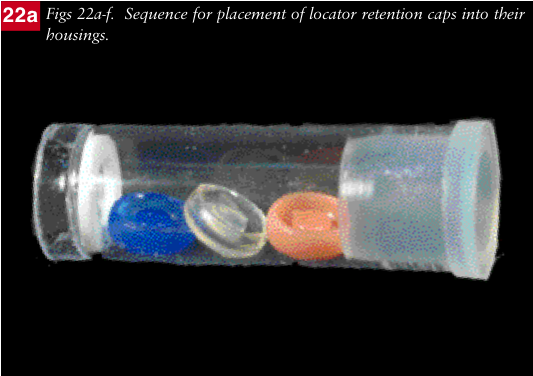
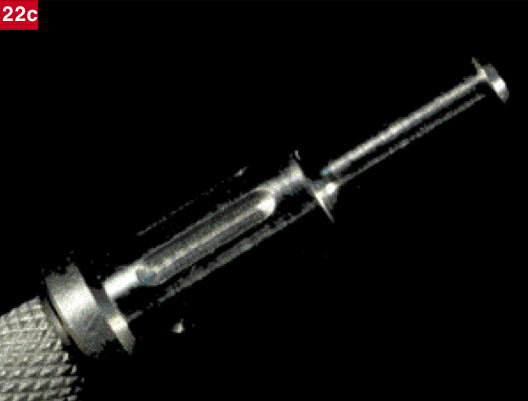
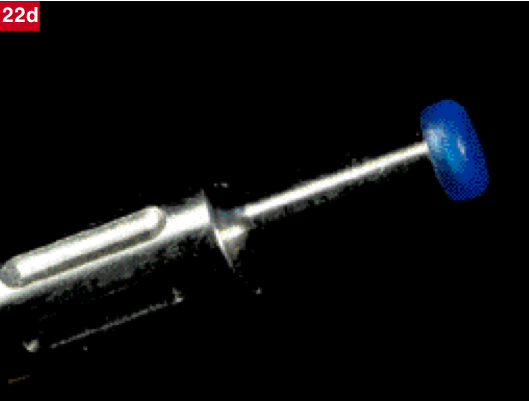
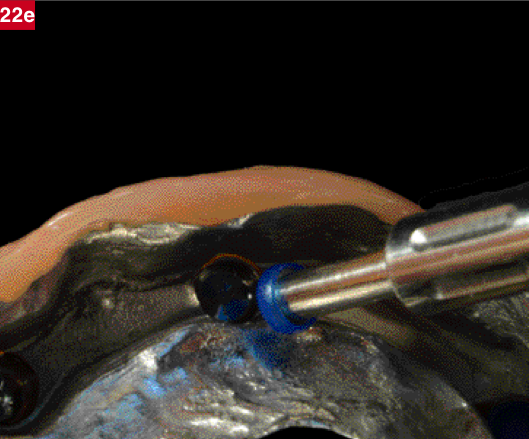
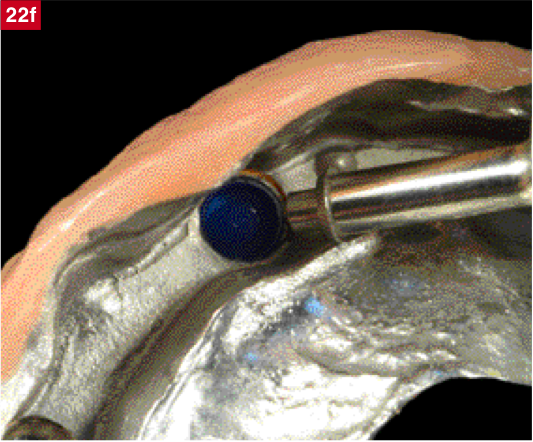
The upper denture was finally trimmed and polished and the locator retention caps inserted (Figs 22a-f).
The acrylic over the screw holes in the lower bridge were carefully drilled out to expose the silicone putty which was then removed to access the screws. The structure was then removed from the model trimmed and finally polished.

Fitting
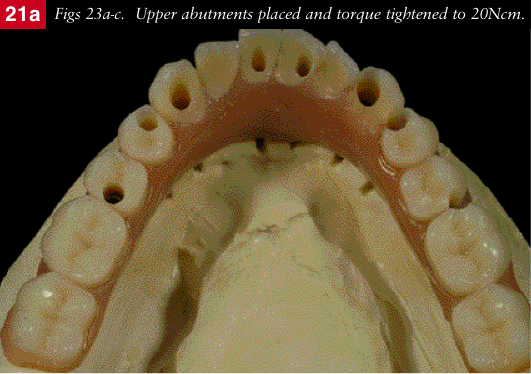
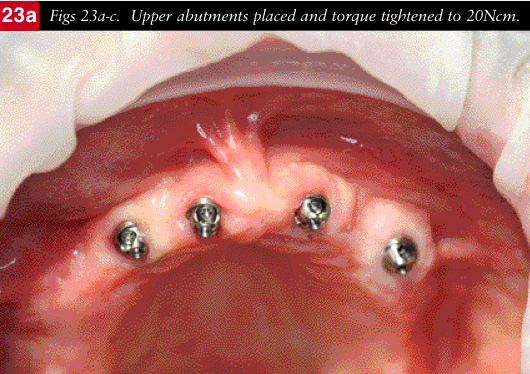
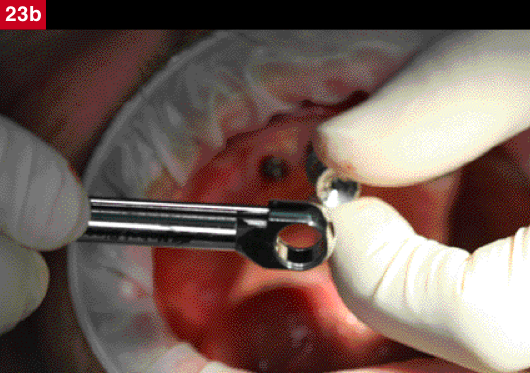
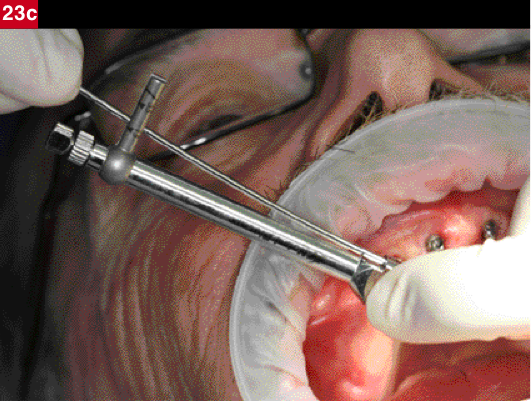
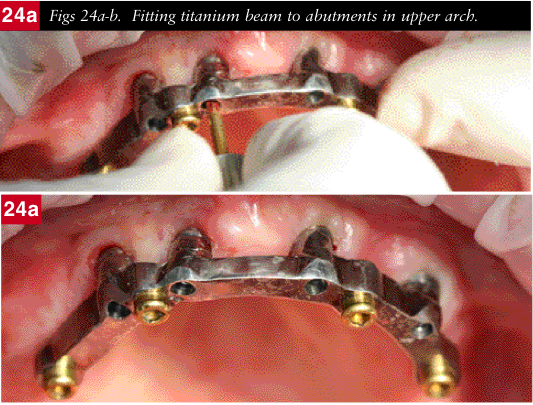
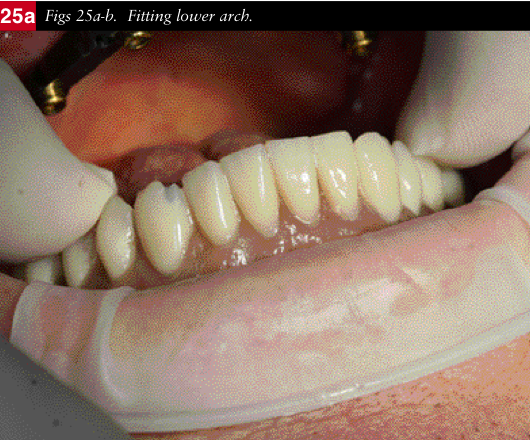
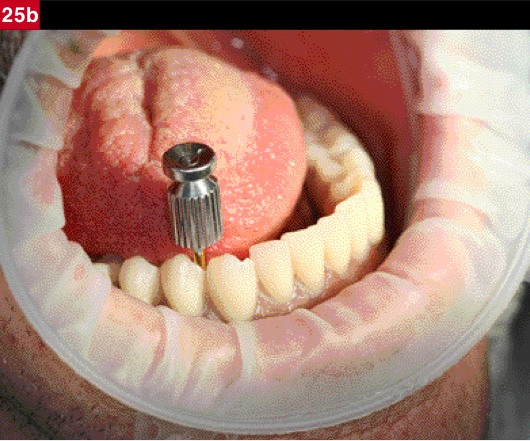
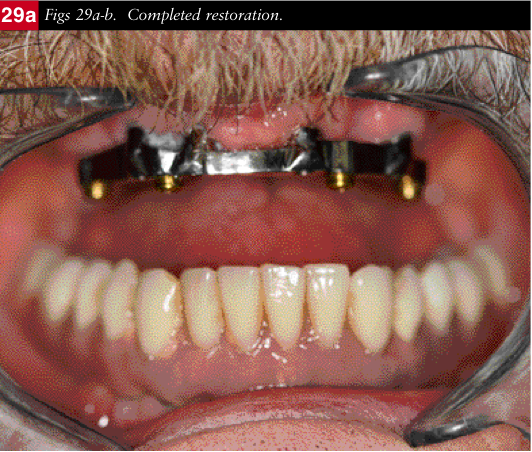
The upper healing caps were removed and the abutments screwed in and torque tightened (Figs23a-c). The titanium beam was then screwed to the abutments and torque tightened (Figs 24a-b). The upper denture was then seated over the beam. The lower bridge was screwed into place and tightened to 25Ncm (Figs25a-b).
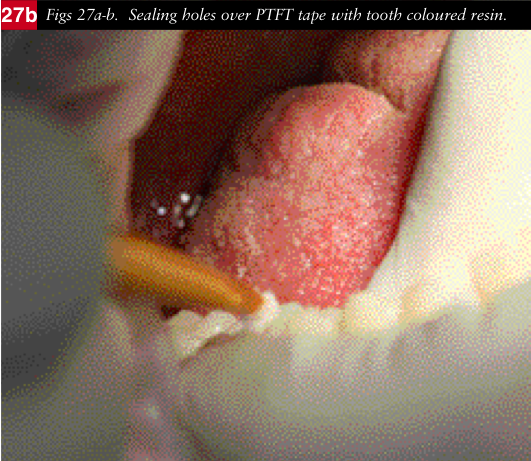
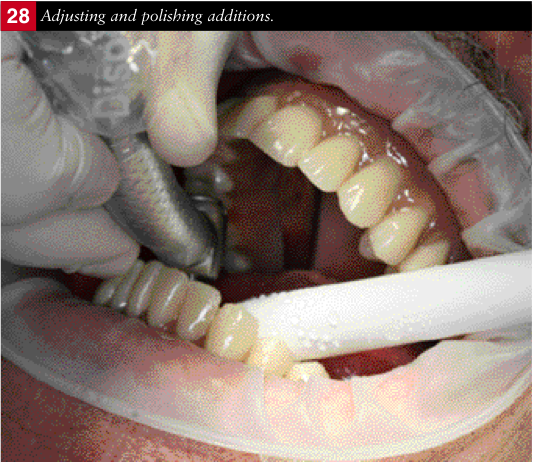
The holes were then partially filled with ptfe tape (Figs26a-c) to ensure ease of access to the screws, if necessary, at a future date and then covered with tooth coloured resin (Figs 27a-b), before finally being adjusted and polished (Fig 28).



Epilogue
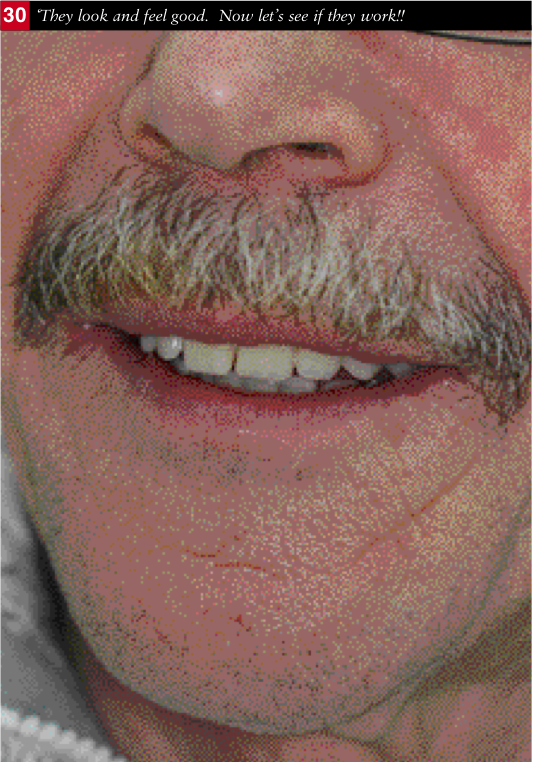
I lived up to my side of the bargain. Allen is now dentally fit, pain free, comfortable, stable and able to eat anything. He is delighted with the aesthetics of his new smile and only wished he had found me years earlier.
As for our kitchen……… (Fig 31).
My sincere thanks to Dr Zaki Kanaan, Dr Omid Sobhani and John Davies for their assistance in the management and treatment of Allen’s reconstruction.

































































































































































































































































